RCUK Quality Standards Group for Care and Rehabilitation of Cardiac Arrest Survivors and Key Supporters
|
Michael Bradfield |
Resuscitation Council UK |
Director of Clinical and Service Development |
|
Emily Carter
|
University Hospitals Dorset NHS Foundation Trust |
Clinical Specialist Physiotherapist |
|
Bernie Cleland |
RCUK Survivors and Co-Survivors Forum |
Cardiac arrest survival key supporter |
|
Julianne Collins |
University Hospitals Dorset NHS Foundation Trust |
Clinical Specialist Occupational Therapist |
|
Jonathan Goodfellow |
Wales Cardiac Network |
National Clinical Lead |
|
Natalie Graham |
Stockport NHS Foundation Trust |
Cardiac Rehabilitation Co-ordinator |
|
Kirstie Haywood |
University of Warwick |
Professor of Health Outcomes |
|
Vicky Joshi |
Glasgow Caledonian University |
Lecturer in Physiotherapy |
|
Asad Kayani |
RCUK Survivors and Co-Survivors Forum |
Cardiac arrest survivor |
|
Thomas R Keeble |
Essex Cardiothoracic Centre, and Anglia Ruskin School of Medicine, UK |
Consultant Cardiologist and Associate Professor |
|
Stephanie Leckey |
Northern Ireland Ambulance Service |
Community Resuscitation Lead |
|
Lisa MacInnes |
Save a Life Scotland |
Director |
|
Fiona Maclean |
Welsh Ambulance Services NHS Trust |
Community Involvement and Engagement Manager |
|
Stuart Menzies |
RCUK Survivors and Co-Survivors Forum |
Cardiac arrest survivor key supporter |
|
Marco Mion |
Essex Cardiothoracic Centre, and Anglia Ruskin School of Medicine, UK |
Principal Clinical Psychologist |
|
Naomi Reeves |
Resuscitation Council UK |
Clinical Lead |
|
Julie Starling |
Save a Life Cymru |
Clinical Out-of-Hospital Cardiac Arrest Programme Manager |
|
Paul Swindell |
Sudden Cardiac Arrest UK and RCUK Survivors and Co-Survivors Forum |
Trustee (SCAUK) and Cardiac arrest survivor |
|
Victoria Wragg |
Resuscitation Council UK |
Clinical Lead |
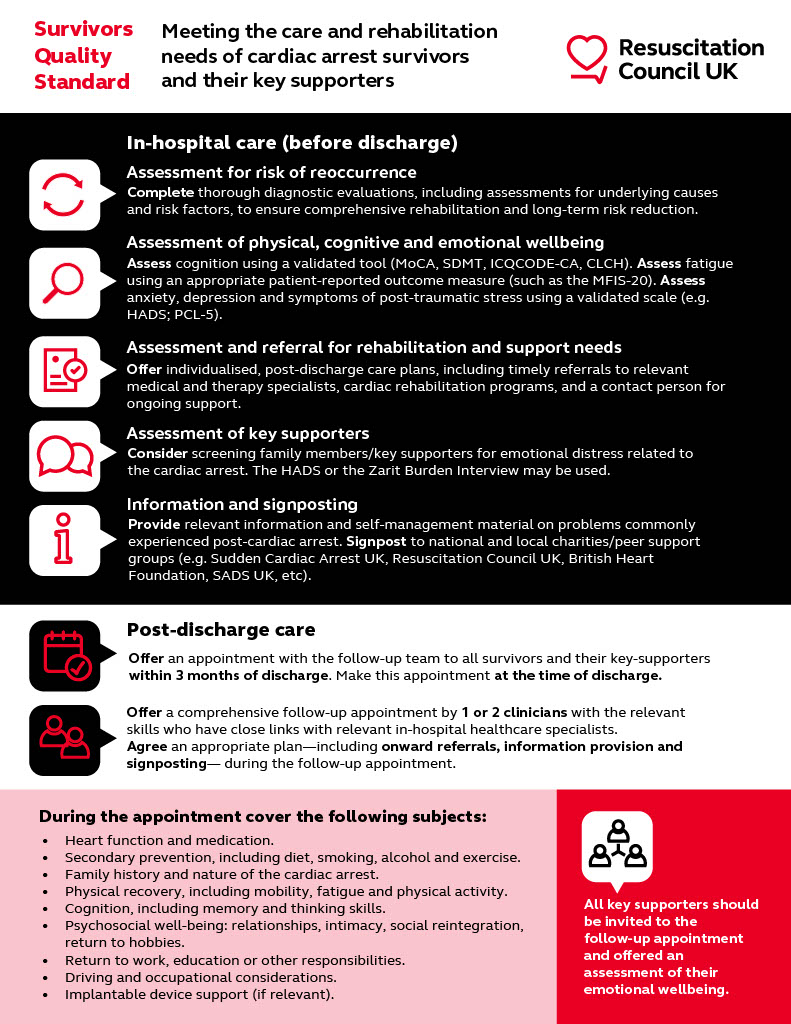
Meeting the care and rehabilitation needs of cardiac arrest survivors and their key supporters
Cardiac arrest affects tens of thousands of people in the UK every year. Although circumstances may differ – with some people experiencing a cardiac arrest in the community and others in healthcare settings – survival always depends on life-saving interventions such as early recognition, calling for expert help, cardiopulmonary resuscitation and defibrillator use. Survival and recovery can be further improved via advanced life support, post-cardiac arrest care, rehabilitation and follow-up. Existing quality standards currently cover resuscitation practice and training in different settings but are not specific to rehabilitation and the survivor’s journey post-hospital discharge.
Survivor
We use the term ‘survivor’ here to describe any individual who has been successfully resuscitated after a cardiac arrest and is not in a prolonged disorder of consciousness or on a specialist neurological rehabilitation pathway. For this Quality Standard, the focus is on Survivors who return home or are living in a community setting.
Key Supporter
The term ‘key supporter’ represents family members, spouses, partners or close friends of cardiac arrest survivors who were impacted by the event (this list is not exhaustive). Some within this group may also identify as ‘co-survivors’. The key supporter term is one that resonated with patient and public involvement (PPI) partners as it reflects both family members as well as those that may not be related but are close to the survivor.
This quality standard relates to the recovery and rehabilitation of survivors of cardiac arrests that happened both in-hospital and out-of-hospital, irrespective of the cause (e.g. cardiac, respiratory, traumatic, unidentified, etc). The scope does not cover addressing underlying causes of the cardiac arrest. Some patients will survive with little to no impairment, most with mild to moderate but some will require substantial ongoing care. This document covers the period before discharge from the hospital up to the long-term follow-up.
By implementing the measures within this quality standards survivors and their key supporters across the four UK nations will be provided with and will benefit from the following:
-
Access to a minimum standard of post-resuscitation assessment of physical, cognitive and mental health needs before and after hospital discharge and signposting to appropriate services where indicated.
-
Improved quality of service provision regarding the above standards.
-
Improved outcomes following successful resuscitation after cardiac arrest. These may include benefits to their physical, cognitive, and mental health and health-related quality of life.
This document provides a realistic and achievable quality standard for the provision of care and rehabilitation needs of cardiac arrest survivors (the ‘survivor’) and their key supporters.
“True recovery is more than having survived and being grateful.”
RCUK CA Survivors Group participant
Cardiac arrest survivors are a highly heterogeneous population, ranging from those who experience minimal long-term health impairments to those who suffer severe hypoxic brain injury and never return home – e.g., due to persistent disorders of consciousness. Some will have ongoing neuro rehabilitation needs with a dedicated pathway, but many will be considered fit enough for discharge home.
Whilst most survivors are discharged to their usual place of residence, many will have rehabilitation and support needs that impact their long-term health-related quality of life. Following a cardiac arrest, around 50% of survivors have mild cognitive impairment, around 40% report limitations due to physical difficulties, around 70% suffer from fatigue, and 15-30% experience emotional problems.
Whilst significant focus is on the survivor after cardiac arrest, this document also provides standards for the follow-up of key supporters. They may also suffer long-term psychological consequences including anxiety, depression, fear, and trauma due to having witnessed/experienced a traumatic event (during resuscitation and/or hospital stay) and having caregiving responsibilities in the mid to long term. They may also have difficulties transitioning to everyday home life after hospital discharge and suffer a high burden of carer strain due to providing support to the survivors from hospital admission through rehabilitation/recovery and beyond.
Consultations with colleagues in Europe and North America have suggested that the challenge is similar across international healthcare systems. Published data indicate that consistency in standards and availability of dedicated follow-up care pathways remain elusive in the UK, Sweden, Denmark, and the United States; yet all of these settings also offer regionalised examples of effective care pathways. For example, informed by an early intervention study tested with cardiac arrest survivors in the Netherlands, the Essex Cardiothoracic Centre established the first dedicated “Care After REsuscitation” (CARE) Service in the UK in 2016. CARE offers a systematic and specialised review of psychological and cognitive needs, with a focus on societal reintegration. Initial evidence suggests that it is possible to address unmet clinical needs with specialist diagnosis and therapy, resulting in improvements to physical and mental health 6 months after discharge from hospital.
In the US, the NeuroCardiac Comprehensive Care Clinic (N4C) and a parallel initiative – the NeuroCardiac Comprehensive Care for Co-Survivors and Family Members, or N4C-F – is the first interdisciplinary clinic that aims to identify and address any neurocognitive/neurological and psycho-social problem to minimize disability and facilitate reintegration into the community.
The ‘Copenhagen Framework' also advocates for a multi-disciplinary guideline-based approach to improving cardiac arrest pathways that should include diagnostic evaluation, screening of survivors and close family members, discharge planning, and both short-term and long-term follow-up and rehabilitation.
As detailed in Section 1 above, the development group included representatives drawn from cardiac arrest survivors, their partners and key supporters; researchers in survivorship and experts from the fields of cardiology, rehabilitation, physiotherapy, nursing, occupational therapy, neuropsychology, speech and language therapy and community resuscitation. This included people from the four nations of the UK, RCUK and partner organisations and charities. The steering group’s focus was survivor-driven, with key representation from the Sudden Cardiac Arrest UK (SCA UK) charity.
{kind=link}
Assessment for risk of cardiac arrest reoccurrence and interventions to reduce this risk
-
All survivors must receive appropriate diagnostic evaluation of the underlying cause of their cardiac arrest, including appropriate clinical evaluation, imaging, and assessments.
-
Diagnosis and treatment may require onward referral, for example to specialists in managing conditions related to electrophysiology or inherited cardiomyopathy. That should mean that survivors are also considered for other elements of rehabilitation and recovery while their underlying cause is addressed.
-
Identification and management of underlying risk factors (such as cardiovascular disease) should also be addressed as part of their assessment. This may also include diet and exercise referral, not only as part of the cardiac rehabilitation and recovery but as a means of reducing risks for the longer term in those patients for whom this may have been a contributing cause.
-
Survivors with no clear cause of their cardiac arrest identified (idiopathic) and their family members should be considered for additional investigations. There is a dedicated pathway for myocardial infarction as a cause of cardiac arrest, but for those with no such obvious cause, further care is still needed. They should receive the same assessment and referral to rehabilitation as any other cardiac arrest survivor and should not be excluded a-priori from services (e.g. cardiac rehabilitation).
Assessment for rehabilitation and support needs
-
All survivors should be offered a multi-disciplinary assessment of their rehabilitation and support needs. Structured questionnaires such as the Informant Questionnaire of Cognitive Decline in the Elderly Cardiac Arrest version (IQCODE-CA) or the Checklist Cognition and Emotion (CLCE-24) may be used.
-
This should be conducted by clinician(s) who have the skills to assess for rehabilitation and support needs after cardiac arrest (e.g. specialist nurses, physiotherapists, occupational therapists, or clinical psychologists – this list is not exhaustive).
Assessment of cognitive problems
-
Survivors must be screened using an appropriate tool such as the Montreal Cognitive Assessment (MoCA), the Symbol Digit Modalities Test (SDMT) or an equivalent tool that is designed to detect even mild cognitive impairments. Post-cardiac arrest cognitive dysfunction may be subtle in some patients, so routinely screening all patients will ensure this is not missed and provides a baseline for any follow-up assessment.
-
Where the screening tool indicates the survivor has fallen below an agreed level (e.g. < 26 on the MoCA) or the survivor or key supporters report subjective cognitive problems it is recommended that the survivor:
- receives an assessment of ‘functional cognition’ in complex tasks pre-discharge, so survivor and family are aware of any deficits and appropriate strategies including social care if required are put in place before discharge home.
- is referred to an appropriate specialist (e.g. care of elderly, neurologist or intensivist) for a more detailed neuropsychological assessment, as well as involvement of specialist occupational therapy and other disciplines as required to co-create a rehabilitation plan. It is recommended that the neurocognitive examination be conducted by someone with an understanding of post-cardiac arrest aftercare.
Assessment of physical problems
-
Survivors should be screened by appropriate healthcare professionals for physical problems, with further specialist assessment to include mobility, strength, balance, sensation, coordination, or vestibular function as required. Self-reported issues relating to physical function can form part of individual assessment but should not be relied upon as the only means of determining need for further support.
Assessment of fatigue
-
Fatigue is the most common problem reported by survivors. All survivors must be assessed for fatigue. It is recommended to use an appropriate patient-reported outcome measure. Scoring systems may include the Modified Fatigue Impact Scale, Fatigue Assessment Scale or Fatigue Severity Scale although there is not a specific recommendation for cardiac arrest survivors.
-
If initial assessment indicates there are fatigue issues, appropriate referral to a fatigue assessment and rehabilitation service is recommended.
Assessment of emotional wellbeing
-
Screening of emotional problems such as depression, anxiety or post-traumatic stress disorder (PTSD) is recommended for all survivors. Widely used measures such as the Hospital Anxiety and Depression Scale (HADS) and PTSD checklist (PCL5) are recommended.
Referral for rehabilitation and support needs
-
Based on the inpatient assessment, all survivors should have an individually tailored plan for their post-discharge care with referrals made to the most appropriate specialist teams. These include, but are not limited to, medical specialities such as genetic testing, neurology, psychiatry, and therapy specialities such as occupational therapy, physiotherapy, speech and language, and neuropsychology
-
Referral to cardiac rehabilitation programmes is recommended for all survivors regardless of the cause of their cardiac arrest.
-
Referral to rehabilitation/support services should be made before discharge where possible.
-
Survivors should be given the name and contact details of a key person who has a copy of the tailored plan and can assist with referrals to services.
Assessment of key supporters
-
It is recommended that family members or other key supporters are screened for emotional distress associated with the cardiac arrest event, as well as their ongoing role as a carer and supporter. The HADS and the Zarit Burden Interview may be used to this effect.
-
Referral to the key supporter’s own GP, social worker or psychologist may be appropriate.
Information and signposting
-
Before discharge, the survivor and their key supporters should receive relevant information and self-management material on problems commonly experienced post-cardiac arrest, including cognitive, physical, and emotional subjects as well as fatigue, resuming daily activities, driving, returning to work, relationships and sexuality where relevant. This should be in an appropriate format (leaflets, videos)
-
Survivors and their key supporters should be signposted to national/local charities and peer-to-peer support groups, e.g. Sudden Cardiac Arrest UK (SCA UK), Sudden Arrhythmic Death UK (SADs UK), Resuscitation Council UK, British Heart Foundation, and Chest Heart and Stroke Scotland (this is not an exhaustive list, and there are updated links available at www.resus.org.uk).
-
They should have the name and contact details of a key person who can provide information by telephone or email and who also has access to their in-patient assessment and tailored plan for rehabilitation and support.
3-month follow-up
-
It is recommended that the assessment by the follow-up team is completed by one or two clinicians (e.g. specialist nurses, occupational therapists, clinical psychologists - this list is not exhaustive). The team should have close links with relevant in-hospital healthcare specialists such as physiotherapists, speech and language therapists, neuropsychologists, and various medical specialities.
-
It is recommended that the follow-up team works as a single point of contact with a dedicated team of healthcare professionals who have specific knowledge of post-cardiac arrest issues.
-
An appointment with the follow-up team should be offered to all survivors and their key supporters within 3 months of discharge, with the appointment made at the time of discharge.
-
The appointment should be suited to their communication needs, preferably in person- but maybe by telephone or video conference.
-
Survivors should be able to self-refer or be referred by other health professionals including GPs to the follow-up clinic if this has not already been done by the discharging hospital.
-
The following aspects of care and recovery should be covered during the follow-up visit which should lead to an individualised recovery care plan. The plan should be a holistic approach based on the experiences of the survivor and their key supporters, rather than focusing on the domains of healthcare specialties. Recommended subjects covered at the 3 month follow-up, which include Patient Reported Outcome Measures where possible:
-
Heart function and medication for cardiovascular disease.
-
Risk factors for secondary prevention, including diet, smoking, alcohol and exercise.
-
Implantable device support (if relevant).
-
Family history and nature of the cardiac arrest.
-
Physical recovery, including mobility, fatigue and physical activity.
-
Cognition, including memory and thinking skills (assessed using the MoCA, SDMT or a similar standardised test).
-
Psychosocial well-being – including relationships, intimacy, social reintegration, and returning to hobbies and interests.
-
Return to work, education or other responsibilities.
-
Driving and occupational considerations.
-
-
All key supporters (who wish to be involved) should be invited to the follow-up appointment, offered an assessment of their emotional well-being and provided information about managing their well-being and recovery and, if required, how they can support their survivor in their recovery, including signposting to appropriate resources (see section below)
-
Survivors and their key supporters should generally be discharged by the follow-up clinic after an appropriate plan has been put in place and agreed referrals made.
Long term follow-up
For the purpose of these quality standards, ‘long-term’ refers to the period after the initial follow-up (3 months plus).
Be aware that individuals may need to access different information at different time points after the initial follow-up to support them in “making sense” and self-managing their condition. Reasons for survivors/Key supporters to contact the follow-up team for a re-referral likely revolve around information-seeking on specific issues, or the need for counselling (cardiac-arrest-specific counselling services, if available) and how to access this.
-
Survivors and their key supporters should be made aware they can self-refer back to the follow-up clinic if there is a cardiac arrest-related issue that has emerged later on that they would like to be addressed. These referrals should then be screened for ‘appropriateness’ by the ‘follow-up’ team.
-
The ownership for pre-discharge assessment and follow-up care of all survivors must be agreed upon at a local level. For cardiac arrest survivors, there is the potential for confusion as to which speciality or hospital provider will ensure follow-up and rehabilitation.
-
It is recommended that there is a clearly identified role providing leadership at a senior (strategic) level to provide resources for the care of cardiac arrest survivors and this may be determined by the acute care provider’s Resuscitation Committee.
-
Organisations should consider using the services that already exist locally for similar patient groups (post-intensive care, traumatic brain injury, stroke, and cardiac disease) to deliver services for cardiac arrest survivors. Solutions include upskilling existing staff and expanding referral criteria to current services to accept cardiac arrest survivors.
-
Organisations should ensure that healthcare professionals who undertake and interpret standardised assessments receive appropriate training to do so (if required)
-
Appropriate systems should be in place to initiate referrals and escalation pathways to other medical/therapy specialists.
-
Organisations should ensure that there is a nominated recovery programme lead to champion cardiac arrest recovery. This is a key role to oversee the programme at a service delivery (day-to-day) level, from in-hospital assessments to outpatient follow-up.
-
Appropriate space, technical support and facilities should be made available.
-
Organisations should undertake appropriate audit of service delivery.
1. Cardiac Risk in the Young. https://www.c-r-y.org.uk/
2. Sudden Cardiac Arrest UK. https://www.scauk.org/get-support/
3. Sudden Arrhythmic Death UK. https://www.sadsuk.org.uk/
Boyce, L. W., Goossens, P. H., Moulaert, V. R., Pound, G., & van Heugten, C. M. (2019). Out-of-hospital cardiac arrest survivors need both cardiological and neurological rehabilitation!. Current opinion in critical care, 25(3), 240-243.
Bradfield, M., Haywood, K. L., Mion, M., Kayani, A., & Leckey, S. (2024). Not just surviving: Towards a quality standard which meets the care and rehabilitation needs of cardiac arrest survivors and their key supporters. Resuscitation, 198.
Byron-Alhassan A, Collins B, Bedard M, et al. Cognitive dysfunction after out-of-hospital cardiac arrest: Rate of impairment and clinical predictors. Resuscitation. 2021;165:154-60.
Case R, Stub D, Mazzagatti E, Pryor H, Mion M, Ball J, et al. The second year of a second chance: Long-term psychosocial outcomes of cardiac arrest survivors and their family. Resuscitation. 2021;167:274-81.
Christensen J, Winkel BG, Eskildsen SJ, Gottlieb R, Hassager C, Wagner MK. Return-to-work and rehabilitation needs in cardiac arrest survivors: an exploratory cross-sectional study. Eur J Cardiovasc Nurs. 2023;22:328-31.
Cicerone, K. D., Goldin, Y., Ganci, K., Rosenbaum, A., Wethe, J. V., Langenbahn, D. M., ... & Harley, J. P. (2019). Evidence-based cognitive rehabilitation: systematic review of the literature from 2009 through 2014. Archives of physical medicine and rehabilitation, 100(8), 1515-1533.
Cronberg, T., Greer, D. M., Lilja, G., Moulaert, V., Swindell, P., & Rossetti, A. O. (2020). Brain injury after cardiac arrest: from prognostication of comatose patients to rehabilitation. The Lancet Neurology, 19(7), 611-622.
Dainty K, Seaton M, Cowan K, Laupacis A, Dorian P, Douma M, et al. Partnering with survivors & families to determine research priorities for adult out-of-hospital cardiac arrest: a James Lind Alliance Priority Setting Partnership. Resuscitation plus. 2021;7:100148.
Gräsner, J. T., Herlitz, J., Tjelmeland, I. B., Wnent, J., Masterson, S., Lilja, G., ... & Perkins, G. D. (2021). European Resuscitation Council Guidelines 2021: epidemiology of cardiac arrest in Europe. Resuscitation, 161, 61-79.
Haywood K, Dainty KN. Life after cardiac arrest: The importance of engaging with the ‘forgotten patient’. Resuscitation. 2018;128:A1-A2.
Hawkes, C., Booth, S., Ji, C., Brace-McDonnell, S. J., Whittington, A., Mapstone, J., ... & Perkins, G. D. (2017). Epidemiology and outcomes from out-of-hospital cardiac arrests in England. Resuscitation, 110, 133-140.
Israelsson J, Lilja G, Bremer A, Stevenson-Ågren J, Årestedt K. Post cardiac arrest care and follow-up in Sweden–a national web-survey. BMC nurs. 2016;15:1-8.
Joshi, V. L., Borregaard, B., Mikkelsen, T. B., Tang, L. H., Nordström, E. B., Bruvik, S. M., ... & Wagner, M. K. (2024). Observer-reported cognitive decline in out-of-hospital cardiac arrest survivors and its association with long-term survivor and relative outcomes. Resuscitation, 197, 110162.
Joshi, V. L., Christensen, J., Lejsgaard, E., Taylor, R. S., Zwisler, A. D., & Tang, L. H. (2021). Effectiveness of rehabilitation interventions on the secondary consequences of surviving a cardiac arrest: a systematic review and meta-analysis. BMJ open, 11(9), e047251.
Joshi, V. L., Tang, L. H., Kim, Y. J., Wagner, M. K., Nielsen, J. F., Tjoernlund, M., & Zwisler, A. D. (2022). Promising results from a residential rehabilitation intervention focused on fatigue and the secondary psychological and physical consequences of cardiac arrest: The SCARF feasibility study. Resuscitation, 173, 12-22.
Joshi VL, Tang LH, Mikkelsen TB, Nielsen JF, Zinckernagel L, Borregaard B, et al. Does time heal fatigue, psychological, cognitive and disability problems in people who experience an out-of-hospital cardiac arrest? Results from the DANCAS survey study. Resuscitation. 2023;182:109639.
Lilja, G. (2017, February). Follow-up of cardiac arrest survivors: why, how, and when? A practical approach. In Seminars in neurology (Vol. 37, No. 01, pp. 088-093). Thieme Medical Publishers.
Lilja, G., Ullén, S., Dankiewicz, J., Friberg, H., Levin, H., Nordström, E. B., ... & Cronberg, T. (2023). Effects of hypothermia vs normothermia on societal participation and cognitive function at 6 Months in survivors after out-of-hospital cardiac arrest: a predefined analysis of the TTM2 randomized clinical trial. JAMA neurology, 80(10), 1070-1079.
Marijon, E., Narayanan, K., Smith, K., Barra, S., Basso, C., Blom, M. T., ... & Winkel, B. G. (2023). The Lancet Commission to reduce the global burden of sudden cardiac death: a call for multidisciplinary action. The Lancet, 402(10405), 883-936.
Moulaert, V. R., Verbunt, J. A., van Heugten, C. M., & Wade, D. T. (2009). Cognitive impairments in survivors of out-of-hospital cardiac arrest: a systematic review. Resuscitation, 80(3), 297-305.
Mion, M., Al-Janabi, F., Islam, S., Magee, N., Balasubramanian, R., Watson, N., ... & Keeble, T. R. (2020). Care after REsuscitation: implementation of the United Kingdom's first dedicated multidisciplinary follow-up program for survivors of out-of-hospital cardiac arrest. Therapeutic hypothermia and temperature management, 10(1), 53-59.
Mion M, Case R, Smith K, Lilja G, Nordström EB, Swindell P, et al. Follow-up care after out-of-hospital cardiac arrest: a pilot study of survivors and families’ experiences and recommendations. Resuscitation plus. 2021;7:100154.
Mion, M., & Keeble, T. (2023). Supporting patients and families following an out-of-hospital cardiac arrest: Developing a multidisciplinary care pathway and the role of neuropsychology. The Neuropsychologist, (15).
Mion M, Simpson R, Johnson T, Oriolo V, Gudde E, Rees P, et al. British Cardiovascular Intervention Society consensus position statement on out-of-hospital cardiac arrest 2: post-discharge rehabilitation. Interv cardiol: Reviews, Research, Resources. 2022;17.
Nasreddine, Z. S., Phillips, N. A., Bédirian, V., Charbonneau, S., Whitehead, V., Collin, I., ... & Chertkow, H. (2005). The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society, 53(4), 695-699.
National Confidential Enquiry into Patient Outcome and Death (NCEPOD). In Hospital Care of Out-of-Hospital Cardiac Arrests: Time Matters. NCEPOD, 2021.
Noc, M., & Mehran, R. (2022). British cardiovascular interventional society consensus: a huge step towards standardised care for out-of-hospital cardiac arrest in the UK. Interventional Cardiology: Reviews, Research, Resources, 17.
Nolan, J. P., Sandroni, C., Böttiger, B. W., Cariou, A., Cronberg, T., Friberg, H., ... & Soar, J. (2021). European resuscitation council and European society of intensive care medicine guidelines 2021: post-resuscitation care. Resuscitation, 161, 220-269.
Nolan, J. P., Soar, J., Smith, G. B., Gwinnutt, C., Parrott, F., Power, S., ... & Rowan, K. (2014). Incidence and outcome of in-hospital cardiac arrest in the United Kingdom National Cardiac Arrest Audit. Resuscitation, 85(8), 987-992.
Pareek, N., Rees, P., Quinn, T., Von Vopelius-Feldt, J., Gallagher, S., Mozid, A., ... & Keeble, T. R. (2022). British Cardiovascular Interventional Society consensus position statement on out-of-hospital cardiac arrest 1: pathway of care. Interventional Cardiology: Reviews, Research, Resources, 17.
Panchal AR, Bartos JA, Cabañas JG, Donnino MW, Drennan IR, Hirsch KG, et al. Part 3: adult basic and advanced life support: 2020 American Heart Association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2020;142:S366-S468.
Perkins, G. D., Callaway, C. W., Haywood, K., Neumar, R. W., Lilja, G., Rowland, M. J., ... & Nolan, J. P. (2021). Brain injury after cardiac arrest. The Lancet, 398(10307), 1269-1278.
Rojas DA, DeForge CE, Abukhadra SL, Farrell L, George M, Agarwal S. Family experiences and health outcomes following a loved ones’ hospital discharge or death after cardiac arrest: A scoping review. Resuscitation plus. 2023;14:100370.
Sawyer KN, Camp-Rogers TR, Kotini-Shah P, Del Rios M, Gossip MR, Moitra VK, et al. Sudden cardiac arrest survivorship: a scientific statement from the American Heart Association. Circulation. 2020;141:e654-e85.
Southern, C,., Tutton L,, E., Dainty KN et al. The experiences of cardiac arrest survivors and their key supporters following cardiac arrest: a systematic review and meta-ethnography. Resuscitation 2024. Special Edition - Cardiac Arrest Recovery and Survivorship. In press.
Steinbusch CV, van Heugten CM, Rasquin SM, Verbunt JA, Moulaert VR. Cognitive impairments and subjective cognitive complaints after survival of cardiac arrest: a prospective longitudinal cohort study. Resuscitation. 2017;120:132-7.
Viktorisson A, Sunnerhagen KS, Johansson D, Herlitz J, Axelsson Å. One-year longitudinal study of psychological distress and self-assessed health in survivors of out-of-hospital cardiac arrest. BMJ open. 2019;9:e029756.
Wagner, M. K., Berg, S. K., Hassager, C., Armand, S., Møller, J. E., Ekholm, O., ... & Stenbæk, D. S. (2020). Cognitive impairment and psychopathology in out-of-hospital cardiac arrest survivors in Denmark: The REVIVAL cohort study protocol. BMJ open, 10(9), e038633.
Wagner MK, Christensen J, Christensen KA, Dichman C, Gottlieb R, Kolster I, Hansen CM, Hoff H, Hassager C, Folke F, Winkel BG. A multidisciplinary guideline-based approach to improving the sudden cardiac arrest care pathway: The Copenhagen framework. Resuscitation plus. 2024 Mar 1;17:100546
Yaow CYL, Teoh SE, Lim WS, Wang RSQ, Han MX, Pek PP, et al. Prevalence of anxiety, depression, and post-traumatic stress disorder after cardiac arrest: A systematic review and meta-analysis. Resuscitation. 2022;170:82-91.
Zeppenfeld, K., Tfelt-Hansen, J., De Riva, M., Winkel, B. G., Behr, E. R., Blom, N. A., ... & Volterrani, M. (2022). 2022 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: Developed by the task force for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death of the European Society of Cardiology (ESC) Endorsed by the Association for European Paediatric and Congenital Cardiology (AEPC). European heart journal, 43(40), 3997-4126.
Zook N, Voss S, Blennow Nordstrom E, et al. Neurocognitive Function Following Out-of-Hospital Cardiac Arrest: A systematic review. Resuscitation. 2021;170:238-46.