Every second counts: Tackling inequalities in resuscitation
Every second counts: Tackling inequalities in resuscitation
When someone has a cardiac arrest, every second counts, no matter who you are, where you're from or your socio-economic status.
This report warns that socio-economic deprivation, a person’s ethnicity, or cultural background shouldn’t determine whether a person is more or less likely to survive a cardiac arrest. As part of the report, we've commissioned research to understand the views and expectations of people from certain ethnic minority groups in England, around learning and performing CPR. Based on the evidence gathered in the report, we've outlined recommendations to create a CPR-trained society to help close the current inequality gap.
It is not right that your ethnicity, or where you work or live should determine whether you’re more or less likely to survive a cardiac arrest. Neither should geography determine the type of care you receive if you’re lucky enough to survive the ultimate medical emergency.
A cardiac arrest is when the heart suddenly stops beating; a person is immediately unconscious and will die within minutes if not treated quickly. It is not the same as a heart attack – these terms are often used interchangeably, however, they are different. A heart attack occurs when an artery supplying the heart with blood becomes blocked, the person will still be conscious. A heart attack may cause cardiac arrest, particularly in the early stages, but this is not inevitable. Out-of-hospital cardiac arrests (OHCA) affect over 100,000 people per year in the UK.
This report focuses on how socio-economic deprivation, a person’s ethnicity, or cultural background are connected to their chances of surviving a cardiac arrest. It outlines that to address inequalities in resuscitation, we have to focus on those who are most likely to have a cardiac arrest, and least likely to know what to do if they witness someone who has had a cardiac arrest.
Health inequalities are not inevitable. They are avoidable, unfair differences in health between different groups of people. They are inherent in the prevalence, treatment and outcomes of cardiac arrest. The UK lags behind other countries in CPR awareness and currently less than one in ten survive a out-of-hospital cardiac arrest. Simple, lifesaving skills and confidence aren’t yet as widespread as they can and must be. If you live in some of the poorest parts of the UK, or come from a particular ethnic minority group, you may be less likely to survive a cardiac arrest. This is not acceptable. Particular attention and innovative activities must be employed to ensure an equitable improvement in cardiac arrest survival across all nations and all communities of the UK.
We recognise the vital importance of partnership to drive our Charity’s work forward through a tackling inequality in cardiac arrest lens. This requires strategic leadership from central and devolved governments; and successful delivery at regional and local levels will be similarly dependent on healthcare professionals, policy makers working together and playing their respective parts in making these practical and achievable recommendations a reality without delay.
Resuscitation Council UK (RCUK) is the leading authority on resuscitation in the UK. From the evidence gathered within this report, recommendations are made that can close the inequalities gap that currently exists when someone has a cardiac arrest.
To achieve this vision, some of our key recommendations include:
Addressing inequalities in resuscitation must first start with targeted efforts to increase public awareness of a cardiac arrest. As part of ‘Restart a Heart’ month in October every year, we ask that Westminster and the Devolved Governments work in partnership with us to support and fund a public awareness campaign that targets CPR training resources in cardiac arrest hotspot areas (parts of the country with high incidence of cardiac arrest and low CPR bystander rates). Increasing survival rates for people living in more deprived areas, where risk is greatest, and giving them the skills they need to save a life, can only be achieved through partnership. Working with the support of Government at a strategic level will be key to achieving this goal.
Over a third (38%) of UK adults have never undertaken any form of training to learn essential CPR skills. Access to CPR training is not consistent across all segments of the population. This issue is most pronounced in cardiac arrest hotspots. In fact, levels of training are significantly lower for people from ethnic minority backgrounds compared to the UK population. Just 22% received training in the last 10 years, compared with 41% of the UK population in the same period.
Over a third (38%) of UK adults have never undertaken any form of training to learn essential CPR skills.
The UK Government can significantly reduce disparities in CPR training access across occupational and ethnic groups, by legislating for CPR training to be part of the driver licence test, and the DVSA’s Compulsory Basic Training (CBT) for motorcycles and mopeds. Around 180,000 moped and motorcycle drivers take the CBT test annually, which we believe could ensure greater CPR confidence in younger drivers, and many more from underserved communities.
At present, access to CPR training is inconsistent across all segments of the population. Research suggests that professional, managerial and non-manual occupations may be more likely to have been trained than those in manual, unskilled occupations, and the long-term unemployed. Innovative strategies are now required to prioritise CPR training access across certain occupational groups with significantly lower access.
In the UK, 67% of drivers in manual or ‘unskilled’ occupations depend on a private vehicle for transport to work. The United Kingdom should join nearly half of the countries in Europe who teach CPR training through the driving licence test. This public health initiative is low cost and provides a greater foundation of CPR knowledge among the UK population who may not otherwise be trained.
Around 180,000 moped and motorcycle drivers take the CBT test annually, which we believe could ensure greater CPR confidence in younger drivers, and many more from underserved communities.
Data saves lives. The routine collection of comprehensive data that effectively identifies and targets hotspot areas will be invaluable in tackling inequalities in out-of-hospital cardiac arrest. National out-of-hospital cardiac arrest registries are at the heart of successful survival rates across the world. All four nations must continue to commit to a national registry, which collects, analyses and reports data to improve outcomes after a cardiac arrest. Benchmarking in this way is a powerful driver for improvement.
Public-access defibrillation (PAD) is most needed in areas of high OHCA incidence. However, research indicates there is often a mismatch between where a defibrillator is placed and where a defibrillator is needed most. Governments across the United Kingdom must lead prioritising the location of public-access devices in data-identified areas of greatest need. This will be in the poorest parts of the UK and areas with high levels of people from ethnic minority backgrounds. Government defibrillator initiatives should also include a requirement to ensure defibrillators are registered on The Circuit. The Circuit is the national defibrillator network, funded by the British Heart Foundation (BHF), NHS England, Resuscitation Council UK (RCUK) and St John Ambulance (SJA). This will decrease the time to defibrillation in a situation where every second counts.
Governments across the United Kingdom must target publicaccess devices in line with where the data tells us the need is greatest first.
Lord Aberdare (Vice Chair of the APPG on Defibrillators)
I am delighted to endorse Resuscitation Council UK’s (RCUK) report, identifying the inequalities that exist in resuscitation across the United Kingdom, and how to address them. Tackling inequalities in resuscitation requires collaboration from various stakeholders, but this ambition cannot be achieved without government action. RCUK have listened to people affected by inequality in cardiac arrest and there is a determination to ensure that in the ultimate medical emergency, everyone has an equal chance of survival.
The next Parliament presents an opportunity to drive up the UK’s cardiac arrest survival rates to be among the best in the world. Resuscitation, defibrillation and CPR have recently risen up the agenda of all political parties. However, while progress is being made, there are several low-cost measures where further change is needed to save more lives.
Together, let us strive for a future where the compassion and courage of ordinary citizens can turn the tide against out-of-hospital cardiac emergencies. Government action will be vital in bringing together these public acts.
A resuscitation attempt is carried out by the emergency services on approximately 34,000 people a year. Most (around 80%) out-of-hospital cardiac arrests (OHCA) occur in the home, and around half are witnessed by another person. Early recognition, CPR and defibrillation significantly improves the chance of survival. Resuscitation Council UK is committed to giving people, across the UK, the skills they need to save a life.
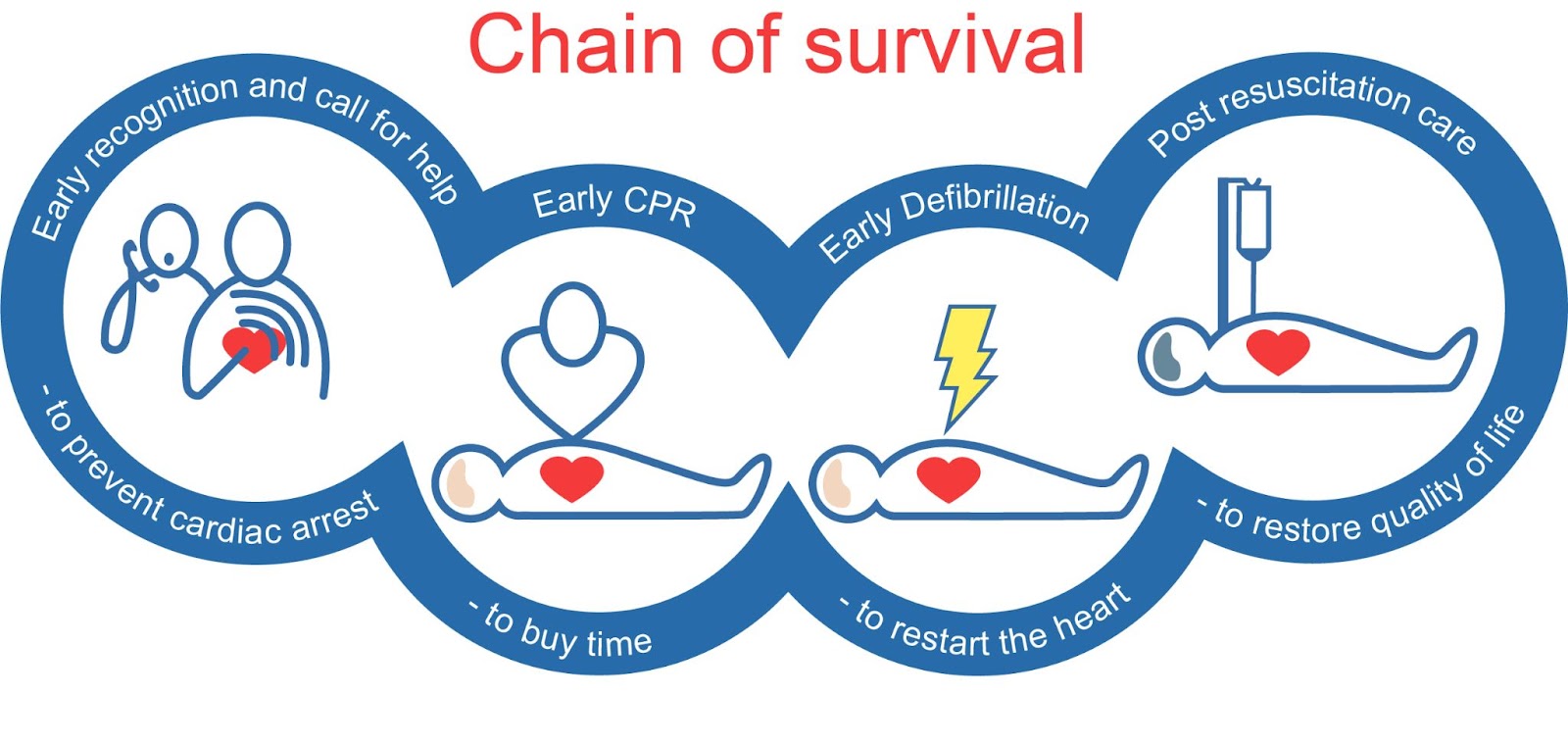
The Chain of Survival describes the crucial elements required to save a life when someone is in cardiac arrest. The first link in the chain is the immediate recognition of cardiac arrest and calling for help. The second is the prompt initiation of CPR. The third is performing defibrillation as soon as possible. The fourth is optimal post-resuscitation care.
Chain of survival
Figure 1: The Chain of Survival outlines a series of events that need to happen quickly for someone to recover after having an outof-hospital cardiac arrest OHCA. Image Credits: European Resuscitation Council.
80% of out-of-hospital cardiac arrests (OHCA) occur in the home.
The cardiac arrest ‘Chain of Survival’ is only as strong as the weakest link in the chain. As each link in the chain of survival improves in strength, so do outcomes in out-of-hospital cardiac arrests. Addressing the inequalities that exist in the earliest stages of the chain of survival is key to achieving this vision. This is why it is paramount that people in underserved communities, who are at highest risk, must have access to educational and training resources that are co-produced with them around how to identify and respond to an out-of-hospital cardiac arrest.
This information must be tailored to a variety of diverse audiences with differing cultural and language needs. Only with the strategic support and attendant resources available through government can we successfully target CPR training and defibrillator awareness resources in cardiac arrest hotspot areas. This could best be achieved by supporting existing initiatives, like the multi-partner, UK-wide initiative, Restart a Heart. This will make sure as many people as possible know how to save a life in areas where cardiac arrest risk is greatest.
Resuscitation Council UK is campaigning to expand the ‘Chain of Survival’ so that a final link in the chain of survival emphasises the right of recovery for survivors of cardiac arrest.
At present, survivors of cardiac arrest have significantly reduced quality of life, due to a lack of aftercare. Across the UK, survivors are not being assessed for their health and social care needs beyond hospital.
A programme of rehabilitation, targeted to the individual’s needs, improves quality of life, is cost effective, and can reduce hospital readmissions.
40-year-old Asad Kayani had been training for the Half Marathon in Birmingham, having completed marathons previously. The day after his training, on 6 March 2022, Asad met his friends from work, to play a game of five a side football. He was not expecting to wake up in hospital. Were it not for the presence of two hospital medics, he might not have woken up at all.
With no previous health conditions, he began walking back to the football facility and collapsed. He has no recollection of the three days before his cardiac arrest.
Thankfully, the team playing football with him had two players who were medics. They rushed over and started performing CPR.
Asad said:
“Bystander CPR rates are low in our country. I have come to realise this particularly among underserved ethnic minority groups. It is important that everyone learns CPR. It could happen to anyone at any time – I am living proof of that.”
“At present, there are significant barriers in accessing CPR training for certain communities, meaning they are less prepared in the event of an out-of-hospital cardiac arrest.
“I want to empower my community to take an active role in saving lives. As an Asian British man I would like to highlight this, especially for that demographic. Engaging influential community members or institutions can play a pivotal role in embedding the importance of learning CPR and fostering a sense of responsibility to respond effectively during cardiac emergencies”.
Language barriers and cultural beliefs can exacerbate inequalities in resuscitation, particularly in underserved communities where English may not be the primary language.
38% of UK adults have never undertaken any form of training to learn essential CPR skills.
Women are less likely to receive CPR, and have lower survival rates at each successive stage of care.
Several factors influence the inequalities present in resuscitation across the United Kingdom. These include but are not limited to:
Ethnicity:
Evidence confirms that out-of-hospital cardiac arrest disproportionately affects people from certain ethnic minority backgrounds. This is because, OHCAs or out-of-hospital cardiac arrests are most commonly trigged by an existing medical condition, and the risk factor of cardiovascular disease is often connected to incidence of cardiac arrest. Research shows that a person’s ethnicity puts them at increased risk of cardiovascular disease. Subsequently, this places them at higher risk of having a cardiac arrest.
Research commissioned by Resuscitation Council UK confirms that CPR training is significantly lower in some minority ethnic backgrounds than the rest of the UK population. It is also noted that interest in CPR training among these communities appeared to be higher than the rest of the UK population.
Socio-economic status:
A person’s socio-economic status has direct influence over their chances of having an outof-hospital cardiac arrest, and of having one at a younger age. Poverty, poor diet, higher incidence of smoking and higher rates of mental illness are all associated with higher incidence of cardiac arrest.
Low socio-economic status means a person could be less likely to receive bystander CPR during a cardiac arrest, less likely to be near an accessible defibrillator, and ultimately, less likely to survive. Research shows that people from lower socioeconomic backgrounds are less likely to be trained in CPR, and less confident to perform CPR. Bystander CPR can double the chance of survival from OHCA, yet it is performed less often in deprived communities. Deprived communities are doubly disadvantaged.
Public-access defibrillators are urgently required in areas where out-of-hospital cardiac arrests occur most frequently. However, research indicates that across the United Kingdom, defibrillators are often disproportionately placed in wealthier areas, with lower cardiac arrest prevalence. This contrasts with poorer parts of the country where cardiac arrest events are higher. The UK Government must target public-access devices in areas of high OHCA incidence, to increase the chance of survival in these communities. Access to life saving devices should not be a postcode lottery.
Age and gender:
Studies suggest that older adults and women may be less likely to receive timely CPR from bystanders compared with younger adults and men. Women are less likely to receive CPR, and have lower survival rates at each successive stage of care. Resuscitation Council UK encourages people who witness a person who is unconscious and not breathing normally to take immediate action to intervene, irrespective of the gender of the person.
Disability:
An estimated 16 million people in the UK have a disability. People with disabilities have poorer health outcomes, and experience more limitations in everyday functioning than the rest of the population due to health inequities. We need greater research focused on resuscitation education disparities in disability, to ensure the unrestricted access of people with disabilities to CPR training.
Cultural and language barriers:
Language barriers and cultural beliefs can exacerbate inequalities in resuscitation, particularly in underserved communities where English may not be the primary language. Misunderstandings about CPR or fear of causing harm during resuscitation attempts may also prevent some individuals from doing it.
Engaging influential community members or institutions plays a pivotal role in reducing inequalities in resuscitation, by embedding the importance of learning CPR and fostering a sense of community responsibility to respond effectively during cardiac emergencies.
CPR training access:
Over a third (38%) of UK adults have never undertaken any form of training to learn essential CPR skills. Furthermore, access to CPR training is not consistent across all segments of the population.
The United Kingdom requires a multifaceted approach to addressing inequalities in CPR training access. It requires targeted educational campaigns, community-based training initiatives, and legislative efforts to improve access to training in underserved areas.
Bystander confidence:
Sex, age group, marital status, education level, employment, length of time since last training, and number of times trained are associated with greater likelihood of performing CPR. In order to address disparities in CPR confidence, we need policy initiatives that tailor and target interventions to groups least confident to take up CPR training. As CPR confidence increases, so does the likelihood of more people have an equal chance of survival.
Overview of survival rates in the four nations
The below section provides a summary of the signifi cant inequalities in resuscitation across the four nations of the United Kingdom, and the measures being taken to address them.
In 2014, the Out-of-Hospital Cardiac Arrest Outcomes (OHCAO) project established a database which brought together, for the first time, information about people throughout the UK who sustain an out-of-hospital cardiac arrest with a view to improve survival. The current out-of-hospital cardiac arrest survival rate is 7.8%. In 2019, NHS England published ‘Resuscitation to Recovery’, a National Framework to improve cardiac arrest care.
In 2022, there were 98,152 calls attended by the ambulance services in England that were categorised as cardiac arrest. Of those, 34,407 were patients treated by ambulance personnel. This represents those patients who have had a sudden cardiac arrest and for whom it was appropriate for the ambulance service to have started resuscitation and we would expect CPR to be performed.
The NHS Long Term Plan recognises that a key priority is to tackle health inequalities and sets out a plan for “stronger NHS action.” This includes a commitment to reduce unjustified variation in performance and access to health care.
In England, data from national cardiac arrest registries have identified “hot spot” cardiac arrest areas. These are areas with above national average incidence of cardiac arrest and below national average bystander-CPR rates. Greater efforts must be made by the Government to harness this data in order to increase survival outcomes in communities worst affected.
98,152 calls attended by the ambulance services in England that were categorised as cardiac arrest.
34,407 were patients treated by ambulance personnel.
In Scotland, over 3,000 people suffer a cardiac arrest each year. Since 2015, Scotland has made significant progress, achieving the goal of equipping an additional 500,000 people with CPR skills and increasing the survival rate. In 2015, approximately 1 in 20 people survived to leave the hospital after OHCA. By 2022, this number had doubled to nearly 1 in 10.
A key factor in this increase has been the establishment of the Save a Life for Scotland (SALFS) partnership, which brings together the Scottish Government, emergency services, third sector organisations, and academic researchers. SALFS has played a pivotal role in realising the objectives of the OHCA Strategy and has so far trained over 715,000 people in Scotland with CPR skills.
The Scottish Index of Multiple Deprivation (SIMD) is a tool for identifying the places in Scotland where people are experiencing disadvantages across different aspects of their lives. The data has identified that people from more deprived areas in Scotland are almost twice as likely to have an out-of-hospital cardiac arrest. The tool also shows that many affluent areas of Scotland often have the lowest number of OHCA cases, while, at the same time, have the highest levels of bystander CPR intervention and public access to defibrillators.
Figure 4: This shows the distribution of OHCA (blue) and PAD (green) locations by SIMD quintile from August 2019 to March 2022 across Scotland. Quintile 1 (furthest left) represents the most deprived 20% of Scotland’s census data zones, with higher quintile numbers indicating lower levels of deprivation. Source: Resuscitation Research Group’s white paper on ‘Public Access Defi brillators in Scotland’, June 2023.
“Health inequalities, already significant in Scotland, have increased during the pandemic as Covid-19 has had a disproportionate impact on people living in areas of socio-economic deprivation, and on people from Black, Asian or minority ethnic backgrounds. This reinforces the importance of our eff orts to address inequality in outcomes from OHCA.”
According to recent data, only 55% of people in Northern Ireland have received CPR training. Disparities in resuscitation education exist across socio-economic groups, with the least deprived demonstrating a higher rate of training (62%) compared with the most deprived (46%). Rural populations are also less likely to have received training in resuscitation skills, highlighting a concerning gap in preparedness. Data indicates the least deprived population exhibit a higher likelihood of performing CPR (68%) compared with the most deprived population (53%).
Unlike England or Scotland, Northern Ireland does not yet have a comprehensive national registry on out-of-hospital cardiac arrest outcomes, or cardiac arrest hotspot data to identify where health inequalities in cardiac arrest are greatest. Annually, around 1,500 people suffer an out-of-hospital cardiac arrest where resuscitation is attempted. Fewer than 1 in 10 people survive an out-of-hospital cardiac arrest. Northern Ireland began its journey towards improving survival rates for out-of-hospital cardiac arrests with the implementation of the Community Resuscitation Strategy in 2014. The primary objective of this initiative was to empower communities by equipping them with vital life-saving skills.
We ask the Northern Ireland Executive to work with Resuscitation Council UK to create a ‘Save A Life Northern Ireland’ partnership, similar to existing partnerships in Scotland and Wales.
This would bring together key stakeholders in emergency services, third sector organisations, the Northern Ireland Executive and academic researchers. The overall ambition being to help increase the number of people who survive a cardiac arrest in Northern Ireland.
Fewer than 1 in 10 people survive an out-of-hospital cardiac arrest.
Rural populations are less likely to have received training in resuscitation skills.
Between April 2020 and March 2021, the Welsh Ambulance Service NHS Trust (WAST) responded to 6,585 out-of-hospital cardiac arrests (OHCA) of which, 2,791 resulted in a resuscitation attempt. Over 70% of these happened in the home. OHCA data on survival is not routinely collated nationwide. However, a study in Wales and England confirms that patients from Black and Asian ethnicity groups have significantly higher in-hospital mortality from an out-of-hospital cardiac arrest, compared with the white population, despite consistent inpatient management.
Tackling inequality in cardiac arrest and improving the outcomes of OHCA in Wales requires a national registry, which collects, analyses and reports data to improve outcomes. To facilitate this, Save a Life Cymru is working with WAST and the National Data Resource to link pre-hospital and hospital data to inform a registry.
Wales has been actively engaged in tackling OHCA through various initiatives and partnerships. The Out of Hospital Cardiac Arrest Plan, launched in 2017 and the establishment of Save a Life Cymru programme has brought together NHS Wales organisations and the third sector from across the country. A significant milestone was reached when the funding for this life-saving program was increased in 2021.
70% of out-of-hospital cardiac arrests in Wales happen at home.
Currently, the disparities in CPR training access across the UK means many communities are less prepared in the event of an out-of-hospital cardiac arrest. This must change.
Between 2017 and 2022, both the proportions of people trained in resuscitation skills and their self-reported likelihood of using them have increased in the UK. While there has been a 12% increase between this time, still, over a third (38%) of UK adults have never undertaken any form of training to learn essential CPR skills. The United Kingdom requires a multifaceted approach to addressing inequalities in CPR training access. It requires targeted educational campaigns, community-based training initiatives, and legislative efforts to improve access to training in underserved areas.
38% of UK adults have never undertaken any form of training to learn essential CPR skills.
Resuscitation Council UK’s research into CPR training among certain ethnic minority backgrounds in England
RCUK commissioned a survey to understand the views and expectations of people from certain ethnic minority groups in England around learning and performing Cardiopulmonary Resuscitation (CPR).
Fieldwork was conducted in February 2023, in areas with high level of cardiac arrest in London, North East, North West, West Midland and Yorkshire and Humber. The ethnic groups we surveyed include people from Indian, Pakistani, Bangladeshi, African, and Caribbean backgrounds. The survey tool was designed to enable comparisons between this study and the wider population data.
Below is a summary of the insights we found:
Knowledge and experience of cardiac arrests
Over half (57%) claim to have some experience of heart related health problems. And nearly a third (32%) have had first or second-hand experience of cardiac arrest.
Around half (54%) feel confident describing a cardiac arrest and just under half (46%) said they feel confident describing cardiopulmonary resuscitation (CPR). Defibrillator awareness is lower, with only a third (33%) saying that they feel confident describing one.
When asked what action they would take if they witnessed a cardiac arrest, the majority (84%) would be likely to call 999, while half (52%) would perform chest compressions.
Six in ten (59%) said they lacked the knowledge and skills to perform CPR.
This could, in part, be explained by a number of barriers highlighted by research participants. Six in ten (59%) said they lacked the knowledge and skills to perform CPR, and over a third (36%) feared that they would cause more harm.
Similarly, seven in ten (68%) mentioned lack of knowledge and skills when explaining their reluctance to use a defibrillator. Over a third (36%) said they were not sure if they were allowed to use a defibrillator. Some relayed ‘embarrassment if something went wrong’ (31%) as a reason to not use the device. And others worried that an electric shock would be delivered when the person does not need it (23%).
CPR training and defibrillator knowledge:
Levels of training were significantly lower among respondents, compared to the UK population average. Just 22% received training in the last 10 years, compared with 41% of the UK population in the same period. However, the interest in CPR training among these groups appeared to be higher than the rest of the UK population.
Also, they are far less likely to know where their nearest publicly accessible defibrillator is than the rest of the UK population. (70% do not know vs 43% of the UK population where their nearest publicly accessible defibrillator is).
Defibrillator awareness is lower, with only a third (33%) saying that they feel confident describing one.
A key barrier to CPR training is awareness, with 34% saying they do not tend to be aware of training opportunities, and 30% said they had thought this training was only for professionals.
Six in ten (60%) have never been trained in using a defibrillator, with a third (34%) mentioning a lack of awareness of training opportunities.
The research findings indicate that understanding the different types of actions that can be taken when witnessing a cardiac arrest is low. While most would be confident and able enough to call 999, very few would be likely to use a defibrillator.
There is significant fear of causing more harm than good when intervening in a cardiac arrest. Most would prefer to call 999 than try to deliver CPR or use a defibrillator. When you couple this with not knowing where the nearest publicly available defibrillator is, it becomes clear that these communities are significantly vulnerable and at higher risk of not surviving a cardiac arrest.
There are many barriers for some groups when it comes to accessing CPR training. Our research identified a lack of awareness. Other barriers mentioned were cost, time and training location. It is important that training opportunities are provided locally in order to encourage attendance. It was also suggested that training courses are free, or subsidised, making it more accessible for those who cannot afford it.
Engaging influential community members or institutions is key to tacking inequalities in resuscitation. By reaching out to those community leaders who are trusted and influential, the value of learning CPR, and the positive impact it brings, can be effectively promoted.
British Heart Foundation, The Circuit: addressing inequalities underlying access to defibrillators
Research has shown that a data-led approach to understand exactly where defibrillators should be placed, to be most effective, will help reduce these stark inequalities. That is why we are proud to partner with the British Heart Foundation, who lead The Circuit: the national defibrillator network that aims to register all defibrillators in a single database that synchronises with the UK ambulance services.
Along with fellow partners St John Ambulance and the Association of Ambulance Chief Executives, The Circuit provides the NHS ambulance services with vital information about defibrillators across the UK. This is so that in those crucial moments after a cardiac arrest, they can be accessed quickly to help save lives.
The Circuit data shows stark inequalities underlying access to defibrillators
Data from The Circuit shows that deprived areas of the United Kingdom are the most underserved when it comes to defibrillator accessibility. Almost half (44%) of the poorest parts (decile 1) of the United Kingdom have no defibrillator registered on The Circuit. Resuscitation Council UK’s commissioned research also tells us that over a third (36%) of people from ethnic minority groups in hotspot areas said they were not sure if they were allowed to use a defibrillator.
Targeting public-access defibrillators in areas, where the data tells they are needed most and ensuring they are registered on The Circuit will be a significant step in reducing inequality and ensuring everyone everywhere has an equal chance of survival. Early defibrillation within 3–5 min of collapse can achieve survival rates as high as 50-70%. Yet so few people survive an out-ofhospital cardiac arrest in the United Kingdom, in part because defibrillation is not provided quickly enough.
Defibrillator awareness is lower, with only a third (33%) saying that they feel confident describing one. 70% do not know vs 43% of the UK population unsure as to where their nearest publicly accessible defibrillator is.
Figure 7: Defibrillators accessibility across the United Kingdom, based on index of multiple deprivation. Source: British Heart Foundation, The Circuit, 2024.
The Circuit data confirms ethnic minority groups without access to registered defibrillators
There are no defibrillators registered in 56% of areas in the UK where ethnic minority groups are the majority ethnicity (Asian, Asian British, Asian Welsh, Black British, Black Welsh, Caribbean, African). This compares with 31% of areas where White British is the majority ethnicity.
80% of areas where ethnic minority groups are the majority ethnicity (Asian, Asian British, Asian Welsh, Black British, Black Welsh, Caribbean, African) have less than two defibrillators registered. This compares with 54.7% of areas where White British is the majority ethnicity.
In areas where Asian/Asian British/Asian Welsh is the majority ethnicity, there are on average only 4.6 defibrillators per 10,000 population. This contrasts with the on average 13 defibrillators per 100,000, in areas with White British is the majority ethnicity.
Raising public awareness about using a defibrillator is a crucial step to improving survival rates during a sudden cardiac arrest. At present, only 8.5% of defibrillators are used outside of hospitals, indicating a significant gap in accessibility and usage. A defibrillator is essential in increasing survival rates, yet 61% of people say they are not confident enough to use one. Promoting defibrillator awareness will instil confidence and empower individuals to respond swiftly in a situation where every second counts.
The Department for Education recently committed to rolling out 20,000 defibrillators across all schools by the end of the 2022/23 academic year. The DHSC (Department of Health and Social Care) also committed to introduce a £1 million Automated External Defibrillator Fund to support the installation of 1,000 defibrillators in community settings across England.
Government defibrillator initiatives must target areas of high-OHCA incidence and ensure devices are registered on The Circuit, to effectively tackle inequalities in resuscitation and strengthen public access. Where possible, defibrillators must be made available 24/7 for full public access.
Coordinated action is being taken by organisations across the United Kingdom to address the underlying inequalities in resuscitation. In the next section we spotlight the innovative community, policy, and public health initiatives undertaken across the United Kingdom to ensure that as many people as possible have the skills they need to save a life.
Currently, eighty percent of out-of-hospital cardiac arrests happen at home. And just half (51%) of people in the UK would feel confident in responding to a family member suffering a cardiac arrest.
The British Sikh Nurses launched a comprehensive CPR readiness campaign in October 2022, partnering with local gurdwaras to conduct Punjabitranslated CPR workshops. The workshops have empowered 120 participants with life-saving skills.
By 2022, BIMA Lifesavers achieved a new milestone by successfully conducting CPR training in 123 mosques across the UK.
British Islamic Medical Association (BIMA) Lifesavers programme is an innovative and impactful initiative with an aim to close the resuscitation gap in the Muslim community.
It shows the significance of community-led efforts in addressing culturally-sensitive issues and increasing awareness and confidence. By tailoring CPR training sessions in UK mosques, Lifesavers ensure that the programme is culturally appropriate and accessible to the community.
Lifesavers started in 2014 as the ‘Basic Life Support Mosque Project’, teaching life-saving skills in three mosques in London. The project has seen exponential expansion over the years. In 2019, over 840 volunteers came together to teach resuscitation skills to over 40,000 members of the public in 114 mosques. By 2022, Lifesavers achieved a new milestone by successfully conducting CPR training in 123 mosques across the UK.
Through this initiative, thousands of individuals are equipped with life-saving skills yearly. Participants spread awareness within their communities, creating a positive ripple effect.
By recognising the importance of cultural sensitivity and engaging communities directly, Lifesavers demonstrate how community-led initiatives can effectively bridge the gaps in knowledge and awareness, leading to improved healthcare outcomes for all.
The British Sikh Nurses launched a comprehensive CPR readiness campaign in October 2022, partnering with local gurdwaras to conduct Punjabi-translated CPR workshops. The workshops have empowered 120 participants with lifesaving skills and emphasised the importance of prompt CPR and calling for help during cardiac emergencies.
As a result of this new initiative, two gurdwaras now have on-site Automated External Defibrillators (AEDs), highlighting the community’s commitment to CPR readiness. By fostering CPR champions within the community and promoting cultural sensitivity, the campaign is making a significant impact on CPR readiness among Sikhs in saving lives.
"Seva, selfless service, is a fundamental principle of Sikhism, and I’m enjoying that I can extend this seva to saving lives through CPR training."
"CPR is not just a technique; it embodies our Sikh values. It allows me to carry forward the spirit of seva and compassion in every life I can help save."
Evidence shows that increasing CPR knowledge and training in the community is an effective way to empower people to save lives in their local area. Currently, eighty percent of out-of-hospital cardiac arrests happen at home. And just half (51%) of people in the UK would feel confident in responding to a family member suffering a cardiac arrest.
That is why Resuscitation Council UK teamed up with GoodSAM, a platform used to alert people to cardiac arrests in their area, to extend their cardiac arrest responder app to members of the public. Once people have been trained through RCUK’s Lifesaver, they can sign up to GoodSAM as a volunteer cardiac responder, under the lifesavers category. They will then be notified of a cardiac arrest in their local community via their phone.
Previously, responders would have only been health professionals via emergency services. Through this partnership, we now have the lifesaving equivalent of the neighbourhood watch. Through the app, they are alerted via the Ambulance Service to local emergencies through their phone, attending cardiac arrests quickly, before the emergency services arrive.
National strategies to reduce inequalities in resuscitation must draw inspiration from this initiative, by involving not only traditional healthcare professionals, but a variety of community stakeholders in lifesaving interventions. This can bridge gaps in access to immediate life-saving care, particularly in areas where health disparities are greatest. Strategies to increase community-responder involvement must also tailor resources to people where English is not the primary language, and where disparities in technology literacy and digital access exist.
St John Ambulance continue to make strides in addressing health inequalities through its ‘CPR Community Network’. The aim of the network is to equip communities with basic life support skills, so they feel confident to respond and give CPR and use a defibrillator in an out-of-hospital cardiac arrest emergency. The network provides a space to ensure everyone can access lifesaving first aid advice based on their needs or preferred language. The CPR Community Network was created in partnership with NHS England and forms part of wider activity to help increase the survival rates of out-of-hospital cardiac arrests in England, in line with the NHS Long Term Plan.
As the CPR Community Network develops, more resources continue to be created which help eliminate common misconceptions around giving CPR and using a defibrillator. To date, St John’s CPR and defibrillator advice has been translated into multiple languages including Urdu and most recently British Sign Language (BSL). The BSL resources include an impactful video which provides a step-by-step guide explaining how to use 999BSL – a video relay service approved by Ofcom to help deaf and BSL speakers communicate with emergency services - in both BSL and through visual subtitles.
The ‘CPR for Every Body’ project was also created as part of the network to help address inequalities in bystander intervention rates for out-of-hospital cardiac arrests between men and women. Studies suggest that women are less likely to receive CPR than men, though experts aren’t entirely sure why. Some suggest that the fear of touching someone’s chest may be a contributing factor. The resources detail how to give CPR and place a defibrillator on a person with breasts and emphasise that ‘CPR is the same for everybody but not every body is the same’.
Resuscitation Council UK encourages people who witness an unresponsive person who is not breathing normally to take immediate intervening action, irrespective of the gender of the casualty.
The next section provides an overview of the UK’s policy progress in resuscitation, and the legislative ambition required to ensure everyone has an equal chance of survival from a cardiac arrest.
CPR training on the UK’s school curriculum
In countries where basic life support is taught in schools, survival rates from sudden cardiac arrest are significantly (two to three times) higher. This is a key avenue for developing a foundation of knowledge among young people:
A recent study found that schools with public access devices could be effective in treating over two thirds of out-of-hospital cardiac arrests within five minutes. Resuscitation Council UK (RCUK) welcomed the Department for Education’s (DfE) rollout of 20,000 defibrillators across all state schools in England. The Department for Education must now work with these schools to ensure their lifesaving devices are publicly accessible. Otherwise, many communities will be left with little access to a defibrillator outside of school hours.
Governments and local authorities across the United Kingdom have committed to giving every young person CPR training during their school career. Research tells us that access to simple but regular CPR training is most effective in increasing CPR confidence and rates. However, young people across the four nations are leaving school without this lifesaving skill. There is no reliable evidence that this policy change is currently being delivered, in a manner that enables us to address resuscitation inequalities.
CPR training must be tailored to meet the language, cultural, and educational needs of learners, to create a generation of lifesavers in currently underserved communities. Data is a crucial tool for monitoring the progress of this goal.
As the national expert organisation in resuscitation, and the standard-setter in CPR teacher training, RCUK has created several language-accessible animations and resources for teachers to use to teach CPR to their students. We have partnered with British Heart Foundation, St Andrew’s First Aid, St John Ambulance, British Red Cross, the East London Cardiovascular Prevention (ELoPeCVD) group from Barts Health NHS Trust, and others, to develop a webpage that promotes key cardiopulmonary resuscitation (CPR) teacher training resources.
We have created template letters that teachers can send to students’ parents / guardians in advance of teaching this sensitive subject. We have also developed a new animated character “Defib Dani”, who can take visual learners through the simple steps to using a public access defibrillator. Governments across the four nations can work with schools, local authorities, and the Department for Education, to ensure CPR training is being carried out in an equitable manner across all schools. By adopting this strategic partnership, we can give young people from underserved communities their right to become potential lifesavers.
How to address inequalities in resuscitation through the UK’s driver licence tests
At present, access to CPR training is inconsistent across all segments of the population. CPR training through schools and the workplace reaches significant amounts of the general population. Research suggests that professional, managerial and non-manual occupations may be more likely to have been trained than those in manual, unskilled occupations, and the long-term unemployed. Innovative strategies are now required to prioritise CPR training access across certain occupational groups with significantly lower access.
In the UK, 67% of drivers in manual or ‘unskilled’ occupations depend on a private vehicle for transport to work. The United Kingdom should join nearly half of the countries in Europe who teach CPR training through the driving licence test. This public health initiative is low cost and provides a greater foundation of CPR knowledge among the UK population who may not otherwise be trained.
Around 180,000 moped and motorcycle drivers take the CBT test annually, which we believe could ensure greater CPR confidence in younger drivers, and many more from underserved communities.
As part of this initiative, the United Kingdom can significantly reduce disparities in CPR training access across occupational and ethnic groups, by legislating for CPR training to be part of the driving licence test, and the DVSA’s Compulsory Basic Training (CBT) for motorcycles and mopeds. Around 180,000 moped and motorcycle drivers take the CBT test annually, which we believe could ensure greater CPR confidence in younger drivers, and many more from underserved communities.
New strategies are also required to increase access to CPR training for underrepresented occupational groups such as the unemployed. Jobcentre Plus centres provide individuals with training, guidance, and resources to enable job-searchers to find work.
Resuscitation Council UK can offer all drivers and job seekers access to our free ‘Lifesaver’ online training package. This resource will increase familiarity to key resuscitation skills and increase bystander CPR rates in a key part of UK society. It also ensures training is of high quality and adheres to international guidelines and standards, crucial to achieving the desired impact on OHCA survival rate.
Governments and local authorities across the United Kingdom have committed to giving every young person CPR training during their school career.
The United Kingdom’s OHCA survival rates have historically been lower than comparable countries. The reason for this disparity is multifaceted and includes lower levels of public awareness of CPR and defibrillation, low bystander intervention rates, and limited public access to defibrillators.
Resuscitation Council UK can offer all drivers access to our ‘Lifesaver’ online training package.
In this report, we have outlined the most significant inequalities that exist in resuscitation across the United Kingdom. We have examined several ways in which different stakeholders address these inequities and have considered coordinated action that directly engages with underserved communities.
The United Kingdom’s OHCA survival rates have historically been lower than comparable countries. The reason for this disparity is multifaceted and includes lower levels of public awareness of CPR and defibrillation, low bystander intervention rates, and limited public access to defibrillators.
At present, there is a clear social gradient in cardiovascular disease mortality, with more deprived areas across the UK and different ethnic groups experiencing higher mortality rates and therefore more likely to have a cardiac arrest. There is an urgent need for a UK government strategy to reduce the health inequalities that contribute to our low survival rates. We can, and we must, do better.
Creating a CPR-trained society will save more lives, improve public health, and enhance community resilience during emergencies. A modest, but carefully targeted investment of public funds in partnership with NFP partners would deliver a significant increase in survival and positive outcomes and transform the UK into a world leader. Cardiopulmonary resuscitation can become a mechanism to reduce social inequalities, not another measure of them. To achieve this vision, we ask that decision-makers adopt these simple recommendations without delay:
Westminster and the Devolved Governments to support and fund a public awareness campaign, targeting CPR training in cardiac arrest hotspot areas, through ‘Restart a Heart’ month
As part of ‘Restart a Heart’ month in October, we ask that Westminster and the Devolved Governments work in partnership with us to support and fund a public awareness campaign that targets CPR training resources in cardiac arrest hotspot areas (parts of the country with high incidence of cardiac arrest and low CPR bystander rates).
Increase bystander CPR rates through targeted monitoring of CPR training in schools
Governments and local authorities across the United Kingdom have committed to giving every young person CPR training during their school career. However, young people across the four nations are leaving school without this lifesaving skill. Governments across the four nations can work with schools, local authorities, and the Department for Education, to ensure CPR training is being carried out in an equitable manner across all schools.
Legislate for CPR training to be part of driving licence tests
United Kingdom can significantly reduce disparities in CPR training access across occupational and ethnic groups, by legislating for CPR training to be part of the driver licence test, and the DVSA’s Compulsory Basic Training for motorcycles and mopeds. This public health initiative is low cost and provides a greater foundation of CPR knowledge among the UK population who may not otherwise be trained.
Continue to collect ‘out-of-hospital cardiac arrest’ data as part of the national strategy
Data saves lives. The routine collection of comprehensive data that effectively identifies and targets hotspot areas will be invaluable in tackling inequalities in out-of-hospital cardiac arrest. All four nations must continue to commit to a national registry, which collects, analyses and reports data to improve outcomes after a cardiac arrest. Benchmarking in this way is a powerful driver for improvement.
Northern Ireland Executive to work with Resuscitation Council UK to create ‘Save A Life Northern Ireland’
We ask the Northern Ireland Executive to work with Resuscitation Council UK to create a ‘Save A Life Northern Ireland’ partnership, similar to existing partnerships in Scotland and Wales. This would bring together key stakeholders in emergency services, third sector organisations, the Northern Ireland Executive and academic researchers. The overall ambition being to help increase the number of people who survive a cardiac arrest in Northern Ireland.
Prioritise public access to defibrillators in areas of high cardiac arrest incidence
Public-access defibrillators are urgently required in areas where out-of-hospital cardiac arrests occur most frequently. However, research indicates there is often a mismatch between where a defibrillator is placed and where a defibrillator is needed most. Governments across the United Kingdom must target lifesaving devices in line with where the data tells us the need is greatest.
Government and local authority defibrillator initiatives to require registration onto The Circuit
Government and local authority-led defibrillator initiatives must target areas of high-OHCA incidence and ensure their devices are registered on The Circuit, the national defibrillator network, to effectively tackle inequalities in resuscitation and strengthen public access. If a defibrillator is in a cabinet, it should be unlocked. Evidence confirms that, in the use of unlocked cabinets, instances of theft and vandalism are rare. Unlocked cabinets allow immediate access to a defibrillator in a situation where every second counts.
Target CPR training resources for underrepresented occupational groups
New strategies are required to increase access to CPR training for underrepresented occupational groups such as the unemployed. Jobcentre Plus services provide individuals with training, guidance, and resources to enable job-searchers to find work. Resuscitation Council UK requests that the next UK Government offers all jobseekers access to a ‘Lifesaver’ online training package.
"Research from Resuscitation Council UK shows that access to AEDs is not fairly distributed across the income and ethnic distribution of England. I hope that the Minister can address that point and tell us what the Government are doing to tackle these stark examples of health inequality." - Shadow Minister Abena Oppong-Asare (Westminster Hall debate, 2023)
"Less affluent areas face inequality in their cardiac arrest survival prospects, as those who live in more disadvantaged areas are more likely to suffer arrests. We need the Government to take urgent action, so that people are not at greater risk of dying from a cardiac arrest just because of where they live." - Stephanie Peacock, MP (Westminster Hall debate, 2023)
"Learning from countries such as Norway and Denmark—where survival rates are more than double ours, which is below 10% — will the Government extend cardiac first aid training to part of the driver’s licence, to all public sector workers, and to those attending jobcentres?" - Baroness Finlay of Llandaff (House of Lords, 2023)